
Knee Pain Without the Scalpel: Modern, Evidence-Based Options for Australians (2025)
Published by Dr Oliver Khoo at Thursday, June 12, 2025
Tags: Knee, Medical Professionals
Osteoarthritis tops the list. The Australian Institute of Health and Welfare estimates that 8.3 % of the population lives with OA, with the knee the most frequently affected joint. OA now makes up 20 % of the nation’s total musculoskeletal disease burden and shows no sign of slowing as our population ages and BMI rises.
Patellofemoral pain (often labelled “runner’s knee”) is the chief non-arthritic cause, with studies showing an annual prevalence of roughly 23 % in adults.
Traumatic injuries (ligament sprains, meniscal tears) matter too, but for most Australians chronic, load-related problems overshadow acute sport injuries once past their twenties.
Current Australian guidance follows a clear hierarchy: start with lifestyle and exercise, layer in pharmacology only as needed, and reserve injections for flares or specific mechanical problems. Here’s what the evidence supports.
Why it matters: The 2024 Clinical Care Standard stresses that imaging isn’t needed to start conservative care; informed self-management is.
Every reputable guideline – RACGP, Osteoarthritis Research Society International (OARSI), and Cochrane reviews – lists structured exercise as first-line therapy, independent of age or X-ray severity.
For every kilogram lost, knee joint load during daily activities drops by roughly 3 kg. Even a 5 % body-weight reduction can noticeably ease pain. Recent Australian GP journal data confirm that heavier patients gain the largest symptom win per kilo shed.
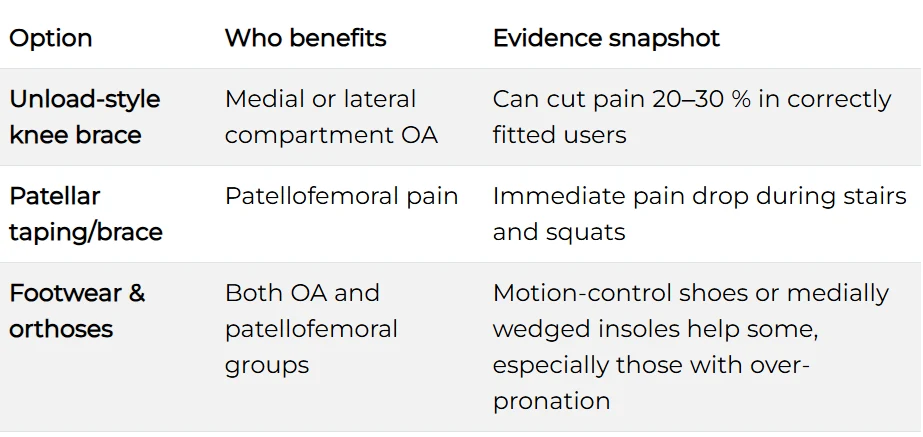
(Use on clinician advice; poor fit can worsen symptoms.)
Australian practice pearl: Ask your GP about a Chronic Disease Management (CDM) plan; Medicare rebates can subsidise physiotherapy while you trial exercise and topical agents.
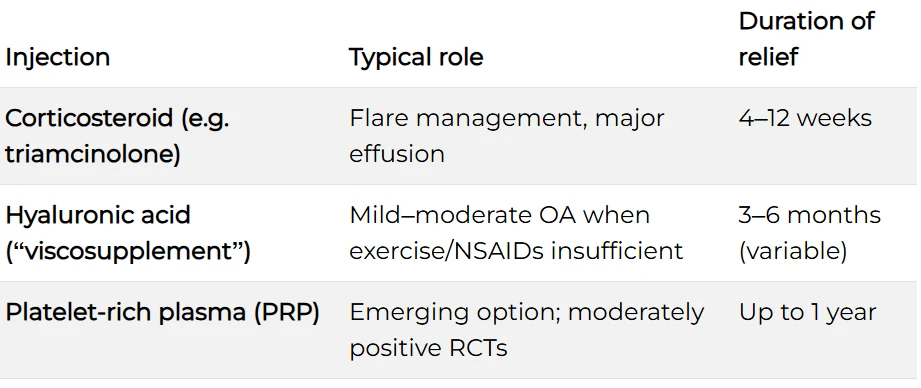
Guidelines place corticosteroid as first-choice for acute inflammatory flare. Viscosupplementation or PRP may be offered when conservative core treatments plateau, but cost and availability vary.
Do I really need an MRI?
Usually not. Most degenerative changes visible on MRI do not alter first-line treatment. X-ray alone suffices when imaging is truly required.
Can I keep running?
If pain remains under a 3/10, swelling is absent and gait stays symmetrical, graded running is fine. Otherwise swap in cycle or pool work until symptoms settle.
How long before I feel better?
Most patients report a meaningful improvement within 6–12 weeks of consistent exercise and weight optimisation, though cartilage changes take longer.
Knee pain doesn’t automatically equal surgery. In 2025, Australians have a robust, evidence-backed menu of non-surgical options—anchored in exercise, lifestyle change and judicious medicine use. Start with the basics, stay consistent, and escalate logically with your GP or physiotherapist’s guidance.