Reverse Shoulder Replacement: Why It Works So Well for Rotator Cuff Damage
Published by Dr Oliver Khoo at Tuesday, December 9, 2025
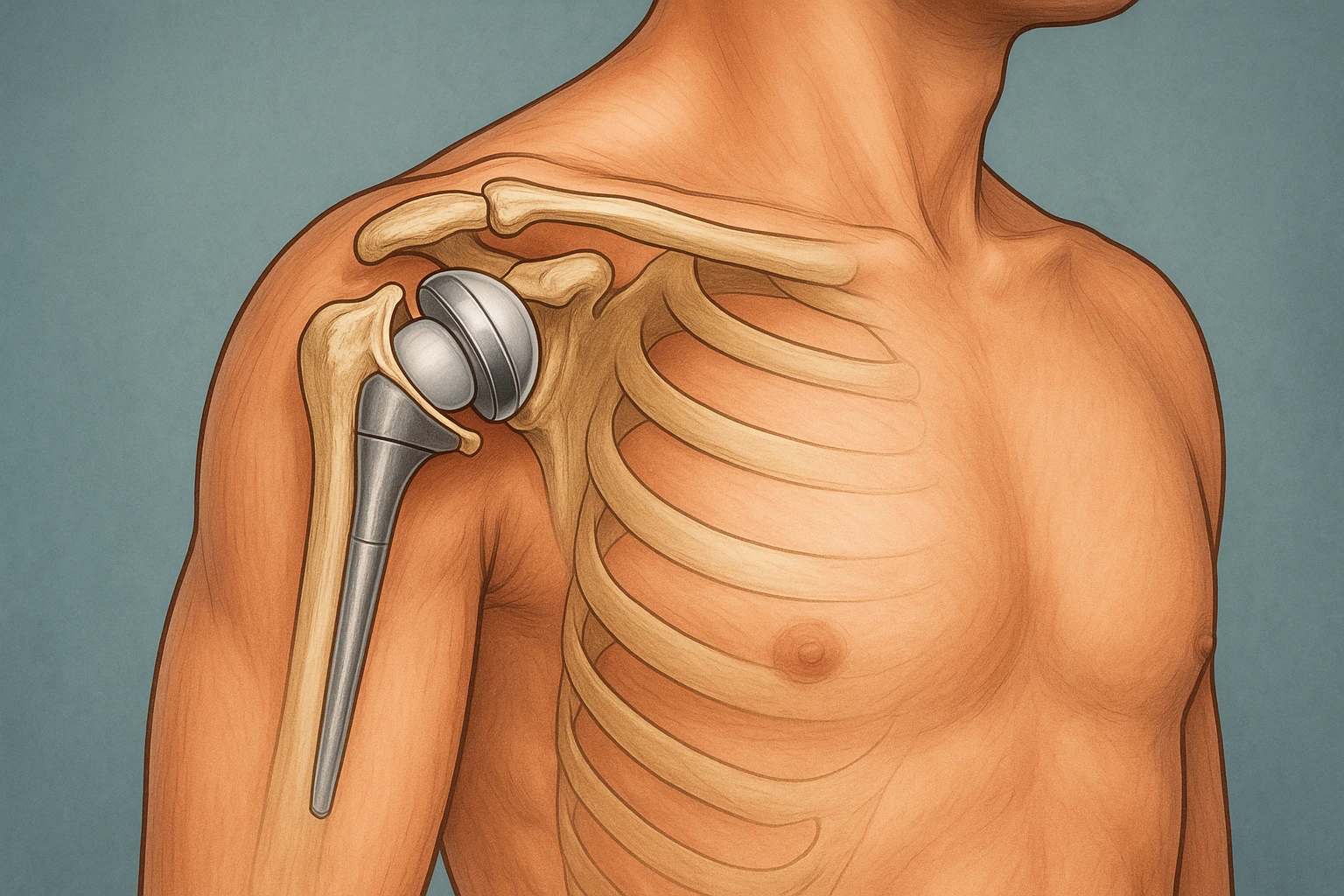
Reverse shoulder replacement has become one of the most successful surgical options for people with advanced rotator cuff tears, long-standing shoulder pain, or severe arthritis that no longer responds to conservative treatments. Unlike a traditional shoulder replacement, it is specifically designed to compensate for a damaged or non-functioning rotator cuff — a common issue as we age or after significant injury.
In recent years, improvements in surgical technique, implant design, and rehabilitation protocols have continued to make this procedure even more reliable for restoring shoulder strength and function. This article explores why reverse shoulder replacement works so well, the biomechanics behind it, the ideal patient groups, and what recovery typically looks like.
The shoulder normally relies on a group of muscles and tendons called the rotator cuff, which helps keep the ball of the joint centred and allows for smooth lifting movements. When the rotator cuff is badly torn or irreparable, this stability is lost, leading to pain, weakness, and limited mobility.
Reverse shoulder replacement changes the joint’s mechanics entirely.
These unique mechanics are the primary reason reverse shoulder replacement is so effective for conditions involving massive or chronic rotator cuff damage.
Reverse shoulder replacement offers several significant advantages for the right patient group. While outcomes vary individually, many patients report dramatic improvements across the following areas:
By removing damaged joint surfaces and restoring stability, most patients experience substantial and lasting pain relief.
Since the deltoid muscle now powers the shoulder, patients regain the ability to lift the arm overhead or perform daily tasks that were previously difficult.
Range of motion often improves considerably, especially for activities like reaching into cupboards, dressing, or grooming.
Reverse shoulder replacement is specifically designed for cases where traditional shoulder replacement would not work due to insufficient cuff strength.
Modern implant designs have improved stability, leading to better long-term durability.
This includes chronic dislocations, failed previous surgeries, and conditions where bone quality is poor.
Reverse shoulder replacement is not recommended for everyone, but it is especially beneficial for the following groups:
When the rotator cuff cannot be repaired, the shoulder becomes unstable and weak. Reverse replacement bypasses this problem by making the deltoid the primary lifting muscle.
This is a type of shoulder arthritis caused by long-term rotator cuff damage. Reverse replacement offers both pain relief and improved function.
Many older patients find this surgery particularly helpful because it works even when the rotator cuff has degenerated over time.
If previous rotator cuff repair or traditional shoulder replacement has not been successful, reverse replacement can be an effective revision option.
In some cases, particularly in older adults, the fracture may be too difficult to fix reliably. Reverse shoulder replacement provides a stable reconstruction.
Recovery is a staged process that focuses on protecting the new joint, gradually improving movement, and rebuilding strength.
Below is a guide to the typical phases many patients follow:
While recovery timelines vary, most patients feel significantly better by the 3-month mark, with continued improvements for up to a year.
Modern implants can last 15–20 years or more, depending on activity levels, bone quality, and overall health. Many patients enjoy long-term pain relief and stable function.
You may not regain the strength you had before your rotator cuff injury, but most patients achieve excellent functional strength for daily living. The goal is improved comfort, mobility, and independence.
Yes. Reverse shoulder replacement is often performed in older patients and is considered very safe when guided by proper assessment and surgical planning.
Low-impact activities — such as swimming, golf, cycling, and gentle gym exercises — are often allowed after recovery. High-impact or heavy lifting activities may be restricted to protect the implant.
As with any surgery, risks include infection, instability, nerve injury, or implant loosening, but these are relatively low. Your surgeon will discuss your individual risk based on your medical history.
You will use your hand and elbow immediately for light tasks, but shoulder use progresses slowly. Most patients begin functional arm use within a few weeks, guided by their physiotherapist.