Shoulder Pain: Joint, Tendons or Nerves? How to Tell the Difference
Published by Dr Oliver Khoo at Thursday, August 28, 2025
Shoulder pain is one of the most common reasons people visit an orthopaedic surgeon. Because the shoulder is such a complex joint, pain can arise from many different structures—bones, cartilage, tendons, ligaments, or even nerves in the neck. Patients often ask: How do I know if my pain is coming from joint degeneration, rotator cuff problems, or nerve irritation?
In this article, I’ll break down the key differences so you can better understand what your symptoms might mean. Of course, every case is unique, and it’s always important to seek a professional diagnosis.
The shoulder joint is designed for mobility rather than stability. It allows us to reach overhead, behind our backs, and across our bodies—more range than almost any other joint in the body. But this flexibility comes at a price: the structures of the shoulder are vulnerable to wear, tear, and strain.
Broadly speaking, shoulder pain tends to fall into three categories:
Understanding the hallmark signs of each can help patients describe their symptoms more accurately to their doctor.
When the shoulder joint itself is the culprit, the pain usually comes from degenerative changes such as osteoarthritis. This occurs when the protective cartilage that lines the joint surfaces wears down, leading to bone-on-bone contact.
Typical symptoms of joint pain include:
In advanced cases, arthritis pain can disturb sleep, making it difficult to lie on the affected shoulder.
A simple tip to distinguish joint pain: If the pain is persistent, dull, and worsens with movement in all directions, the joint itself may be involved.
The rotator cuff is a group of four tendons and muscles that stabilise the shoulder. They are particularly prone to injury and degeneration with age. Tears can be partial or full thickness, and they may result from overuse, trauma, or gradual wear.
Common signs of rotator cuff problems:
Younger patients may injure their rotator cuff through sport or accidents, while older patients often develop tears gradually from tendon degeneration.
Distinguishing feature: If pain is sharp and activity-related, with noticeable weakness in certain movements, a rotator cuff issue is likely.
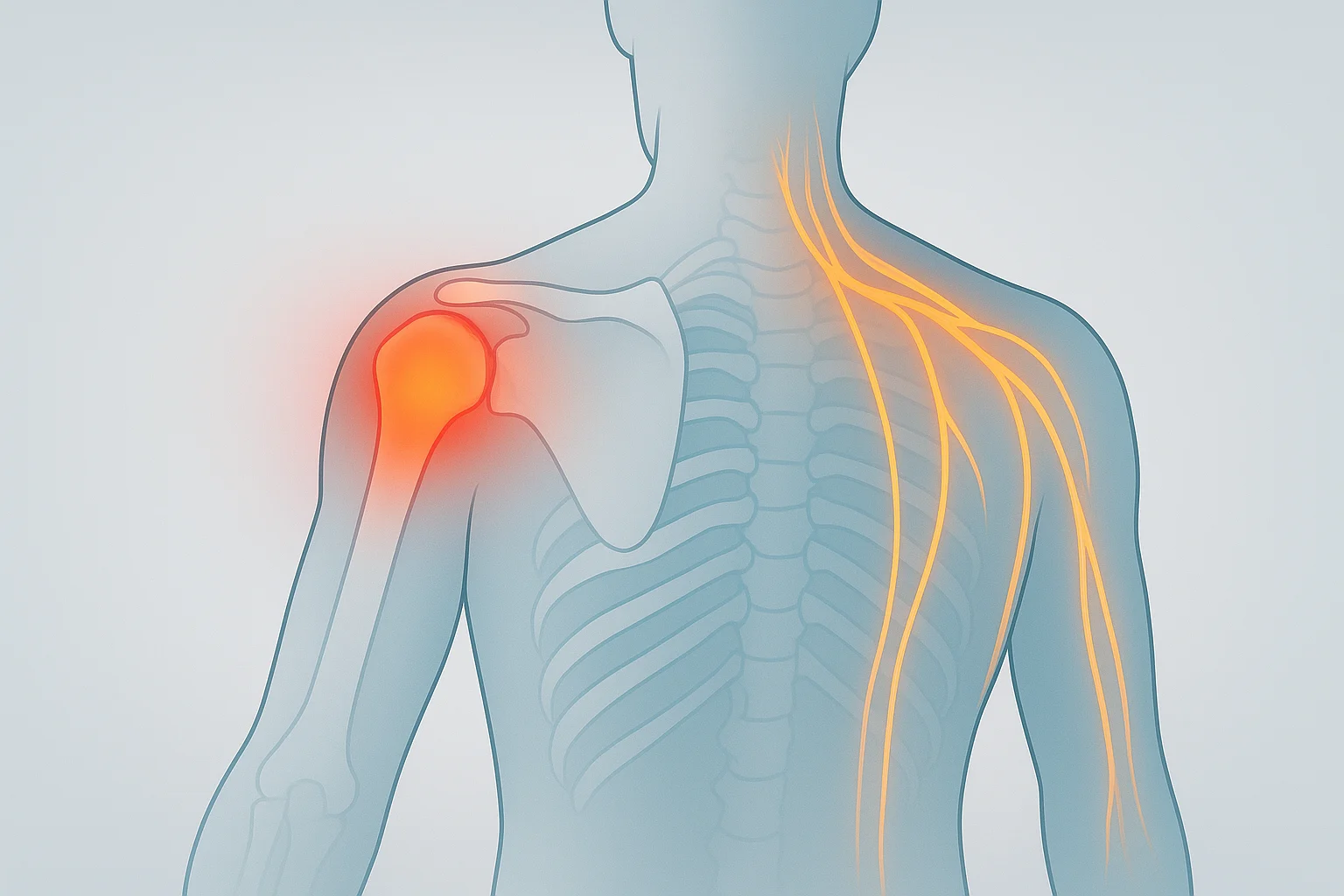
Not all shoulder pain comes from the shoulder itself. Sometimes, the real source is the cervical spine (neck) or surrounding nerves.
When a nerve in the neck is irritated or compressed (for example, by a slipped disc or arthritis in the cervical spine), it can send pain signals down into the shoulder, arm, or even the hand. This is known as referred pain.
Typical features of nerve-related pain include:
Key distinction: If your pain travels beyond the shoulder, especially with tingling or numbness, nerves may be the main culprit.
Doctors don’t rely on symptoms alone—although your description of pain is extremely valuable. A combination of:
helps clarify the diagnosis. Sometimes, diagnostic injections are used—if numbing the joint relieves the pain, the joint is the source. If not, the tendon or nerves may be more likely.
Yes—quite often. An older patient may have mild arthritis and a rotator cuff tear. A person with a stiff neck may also strain their shoulder muscles. Pain sources can overlap, which is why professional evaluation is essential.
Seek medical attention if:
Prompt assessment helps prevent small issues (like minor tendon tears) from becoming larger and more difficult to treat.
Treatment depends on the underlying cause:
Non-surgical care is always the first step, and surgery is reserved for cases where conservative management has not been effective.
1. How do I know if my shoulder pain is serious?
If your pain is severe, persists beyond a few weeks, or is accompanied by weakness, numbness, or tingling, it’s worth seeing a doctor. Sudden inability to move the shoulder after an injury should be treated as urgent.
2. Can shoulder arthritis and rotator cuff tears happen together?
Yes. Many patients have more than one contributing factor to their pain. It’s quite common to see arthritis and tendon degeneration in the same shoulder, especially as we age.
3. Will physiotherapy help with all types of shoulder pain?
Physiotherapy is helpful in many cases, particularly for rotator cuff injuries and mild arthritis. It may also improve posture and reduce strain from nerve-related pain. However, if there is a severe tendon tear or advanced arthritis, surgery may be necessary.
4. What kind of doctor should I see for shoulder pain?
Start with your GP, who can help rule out non-orthopaedic causes. If the problem is clearly within the shoulder joint or tendons, an orthopaedic surgeon specialising in shoulder conditions is best placed to guide treatment.
5. Can shoulder pain ever be heart-related?
Yes, though this is much less common. Pain from the heart (angina or heart attack) can sometimes be felt in the left shoulder or arm. If shoulder pain occurs with chest discomfort, breathlessness, or sweating, seek emergency help immediately.