When Hip Pain Is Actually Coming From the Spine
Published by Dr Oliver Khoo at Thursday, April 16, 2026
Hip pain is often assumed to originate from the hip joint itself, but in many cases, the true source lies in the lumbar spine. Misidentifying the cause can lead to ineffective treatment and prolonged discomfort. Understanding how to differentiate between hip and spinal causes, the role of diagnostic tests and imaging, and when to refer for specialist care is essential for accurate management and better patient outcomes.
Hip pain is a common complaint across all age groups, from active individuals to older adults. While it’s natural to assume the hip joint is the problem, this isn’t always the case. In fact, a significant proportion of what feels like “hip pain” is actually referred pain from the lower back.
The lumbar spine and hip region are closely connected both anatomically and neurologically. Because of this overlap, symptoms can be misleading. Patients may spend months treating the wrong area, delaying recovery.
This article explores how to tell the difference, what tests and imaging can reveal, and how clinicians decide the appropriate referral pathway.
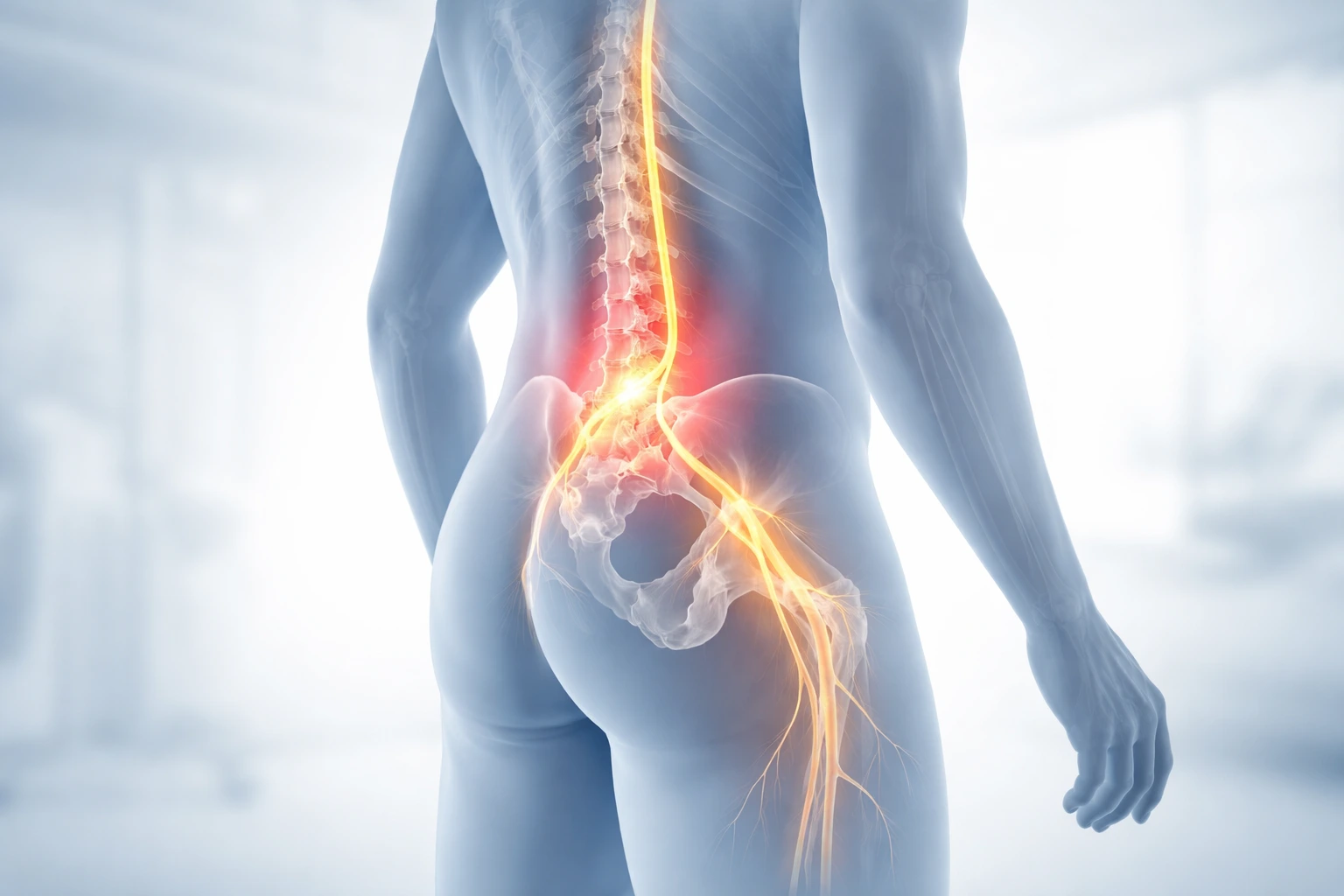
The lumbar spine houses nerves that travel down into the hips, buttocks, and legs. When these nerves are irritated or compressed—such as in conditions like disc bulges or spinal stenosis—the brain can interpret the pain as coming from the hip.
Common spinal-related causes include:
Because nerves supply both the spine and surrounding regions, pain can radiate in patterns that closely resemble hip joint issues.
Differentiating between these two sources is critical for effective treatment. While symptoms can overlap, there are subtle distinctions that can guide diagnosis.
A thorough clinical assessment is the cornerstone of identifying the true source of pain. Experienced practitioners rely on a combination of patient history and physical examination.
No single test provides all the answers, but together they build a clearer picture.
Imaging can support a diagnosis, but it should never be the sole basis for clinical decisions. Findings must always be interpreted alongside symptoms and physical examination.
A skilled clinician will correlate imaging results with the patient’s presentation before making decisions.
Understanding when to refer is just as important as making the initial diagnosis. Not all cases require specialist intervention, but some do.
Early and appropriate referral can significantly improve outcomes and reduce long-term complications.
Treating hip pain as a joint issue when it’s actually coming from the spine can lead to:
On the other hand, identifying the true source early allows for targeted treatment, faster recovery, and better overall results.
If your pain radiates down your leg, worsens with sitting, or is accompanied by numbness or tingling, it may be coming from the spine rather than the hip.
Yes, it’s quite common for patients to have both hip joint degeneration and spinal conditions simultaneously, which can complicate diagnosis.
No. Many cases can be diagnosed through clinical assessment alone. Imaging is typically used when symptoms persist or when serious conditions are suspected.
A physiotherapist or musculoskeletal specialist is often the best starting point, as they can assess both hip and spinal contributions.
Absolutely. Physiotherapy is one of the most effective treatments for spinal-related hip pain, focusing on mobility, strength, and nerve function.
Seek immediate medical attention if you experience severe weakness, loss of bladder or bowel control, or worsening neurological symptoms.